Hip and groin pain are amongst the most common types of musculoskeletal injuries arising from sporting activities. Presently, the evidence for the diagnosis and treatment for athletic groin pain remains unclear due to the inability to scientifically identify its source. This has resulted in a lack of certainty in clinical practice when treating athletic groin pain.
Researchers have classified groin pain using three main entities:
- Adductor-related
- Iliopsoas-related
- Inguinal and pubic-related
Of the above three entities, adductor-related groin pain (ARGP) was the most commonly reported in literature. ARGP is associated with high levels of dynamic lower limb activity i.e. kicking, pivoting and change of direction movements. It is commonly seen in football, ice hockey and rugby athletes — just to name a few.
Let’s explore three of these such protocols which are designed to address ARGP: the Holmich Protocol, the Copenhagen Adduction Protocol and the Rehabilitation Programme Targeted At Intersegmental Control.
The Holmich Protocol
The Holmich protocol is an active physical training program, consisting of a series of therapeutic exercises focusing on improving the strength and coordination of the hip and abdominal muscles.
Researchers have found that the Holmich protocol improved pain and return to sport (RTS) outcomes in athletes with long-standing adductor-related groin pain (LSARGP), when compared to passive Physiotherapy treatment (i.e. stretching, massage and use of electrical modalities).
The Holmich protocol consists of 2 exercise modules over a minimum 8-week treatment period.
Copenhagen Adduction Exercise
It has been demonstrated that eccentric training (i.e. Nordic hamstring exercise) can have preventative effects on hamstring injuries. Eccentric loading optimises the length-tension relationship — to allow the muscle to exert the maximum amount of force at increased absolute muscle length. Hence, the Copenhagen adduction (CA) exercise aims to elicit similar gains in eccentric strength (such as that of the Nordic hamstring exercise), in the management and prevention of athletic groin injuries.
The Copenhagen adduction (CA) exercise is a body weight exercise that specifically targets the hip adductor and abductor muscles. It is a dynamic and high intensity exercise performed to the hip’s outer range of motion. It aims to regain muscular stability in the pelvic and groin area, especially at outer range of motions i.e. during kicking and sprinting. This isolated exercise has shown substantial improvements in eccentric hip adductor (EHAD) strength.
There are 3 levels recommended for relevant age groups and level of play i.e. recreational, intermediate and competitive athletes.
The Holmich protocol and CA exercise demonstrated the effectiveness of an active therapeutic exercise program. Both target hip adductor strength, with an additional focus on eccentric strengthening with the CA exercise. However, the exercises mainly target the hip and abdominal muscles (i.e. hip adductors), thus they could be more beneficial for people with ARGP.
The following exercise sheet contains a description of the exercises included in Holmich and CA exercise protocol.
Click here to download Exercise Sheet
Rehabilitation Programme Targeted At Intersegmental Control
A rehabilitation programme targeting intersegmental control has shown to be effective when assessed using the Hip and Groin Outcome Score (HAGOS), adductor squeeze test and pain-free return to play (RTP).
This programme consists of three levels:
- Address intersegmental control and strength
- Compound movements
- Aim to target multisegmental coordination while building strength
- Involve linear running mechanics and increase linear running load tolerance
- Incorporate rate of force development and running mechanics
- Overstride and dynamic anterior pelvic tilt
- Multidirectional mechanics and the transition back to high intensity sprinting
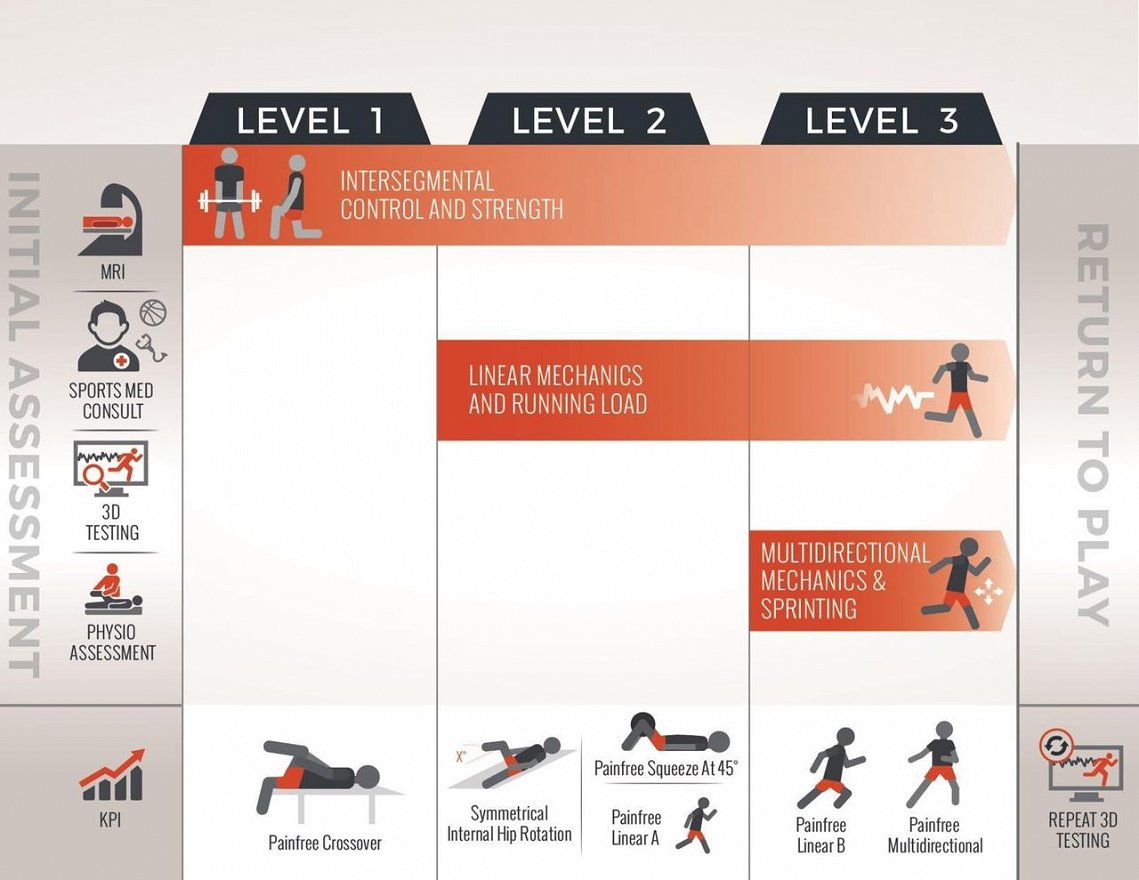
Outline of the intersegmental control rehabilitation program
Unlike the Holmich and CA exercise programs, this is a progressive program. The selection of exercises are highly dependent on the individual’s progress to allow for graded exposure to the exercises and drills. The intersegmental control rehabilitation program is focused on optimising the biomechanics across the entire kinetic chain, to reduce the effect of the external forces on the hip during multidirectional cutting movements.
It was evident that the intersegmental control rehabilitation program improved kinematics and athletic performance for sport-specific movements. Notably, there was a significant improvement in adductor strength (squeeze test), though the program did not include specific adductor strengthening exercises. Hence, this program has shown efficacy in the management and prevention of groin-related injuries, especially for athletes who frequently engage in high-speed movements during sport.
The table below gives a comparison of the above three programmes and the factors which may influence clinical decision making.

How does this inform clinical practice?
Athletic groin pain is notorious for being ‘difficult to treat’. As depicted above, there are several factors to consider when deciding a suitable treatment protocol for various individuals.
Which might be more useful you ask? The Holmich protocol has displayed effectiveness in the treatment of long-standing ARGP. For higher performing athletes with ARGP, the CA exercise may be useful for injury prevention, though results were clinically insignificant. While the effects of conventional strengthening interventions are positive, current literature is unable to ascertain a generalised treatment protocol that can be utilised for all types of hip and groin injuries. However, the coupled effects of adductor strength gains with the intersegmental control program is noteworthy and could provide useful insights for Physiotherapy management.
References:
Hölmich, P. (2007). Long-standing groin pain in sportspeople falls into three primary patterns, a “clinical entity” approach: a prospective study of 207 patients. British journal of sports medicine, 41(4), 247-252.
Hölmich, P., Uhrskou, P., Ulnits, L., Kanstrup, I.-L., Nielsen, M. B., Bjerg, A. M., & Krogsgaard, K. (1999). Effectiveness of active physical training as treatment for long- standing adductor-related groin pain in athletes: randomised trial. The Lancet, 353(9151), 439-443.
Ishøi, L., Sørensen, C., Kaae, N., Jørgensen, L., Hölmich, P., & Serner, A. (2016). Large eccentric strength increase using the Copenhagen Adduction exercise in football: A randomized controlled trial. Scandinavian journal of medicine & science in sports, 26(11), 1334-1342.
King, E., Franklyn-Miller, A., Richter, C., O’Reilly, E., Doolan, M., Moran, K., Strike, S., & Falvey, É. (2018). Clinical and biomechanical outcomes of rehabilitation targeting intersegmental control in athletic groin pain: prospective cohort of 205 patients. British journal of sports medicine, 52(16), 1054-1062.
Weir, A., Brukner, P., Delahunt, E., Ekstrand, J., Griffin, D., Khan, K. M., Lovell, G., Meyers, W. C., Muschaweck, U., & Orchard, J. (2015). Doha agreement meeting on terminology and definitions in groin pain in athletes. British journal of sports medicine, 49(12), 768-774.
Yousefzadeh, A., Shadmehr, A., Olyaei, G. R., Naseri, N., & Khazaeipour, Z. (2018). Effect of Holmich protocol exercise therapy on long-standing adductor-related groin pain in athletes: an objective evaluation. BMJ open sport & exercise medicine, 4(1), e000343.