What is Osgood-Schlatter disease?
Osgood-Schlatter disease (OSD) refers to osteochondritis that occurs at the growth plate of the tibial tuberosity. It is extremely common in adolescents at the time of growth spurt. It is characterized by pain over the tibial tuberosity which is often aggravated by exercise. Diagnosis can be made clinically with a visibly enlarged and tender tibial tubercle. Irregularity and fragmentation of the tibial tubercle can also be seen from radiographs of the knee.

Radiographic appearance of Osgood-Schlatter disease
What causes OSD?
OSD is caused by the repeated contraction of the quadriceps muscles, which may cause softening and partial avulsion of the developing secondary ossification center. It is often associated with repeated force knee extension. This is especially common in sports that involve running, squatting, kicking, and jumping. Examples of such sports include: Basketball, football and gymnastics.
Stages of tibial tuberosity development
There are 3 stages of tibial tuberosity development:
- Sonolucent stage (stage S)
- Characterized by the presence of a large amount of apophyseal cartilage
- Individual stage (stage I)
- Characterized by the presence of apophyseal cartilage within an “individual ossicle”
- Connective stage (stage C)
- Characterized by the connection of the secondary ossification and tibial epiphysis
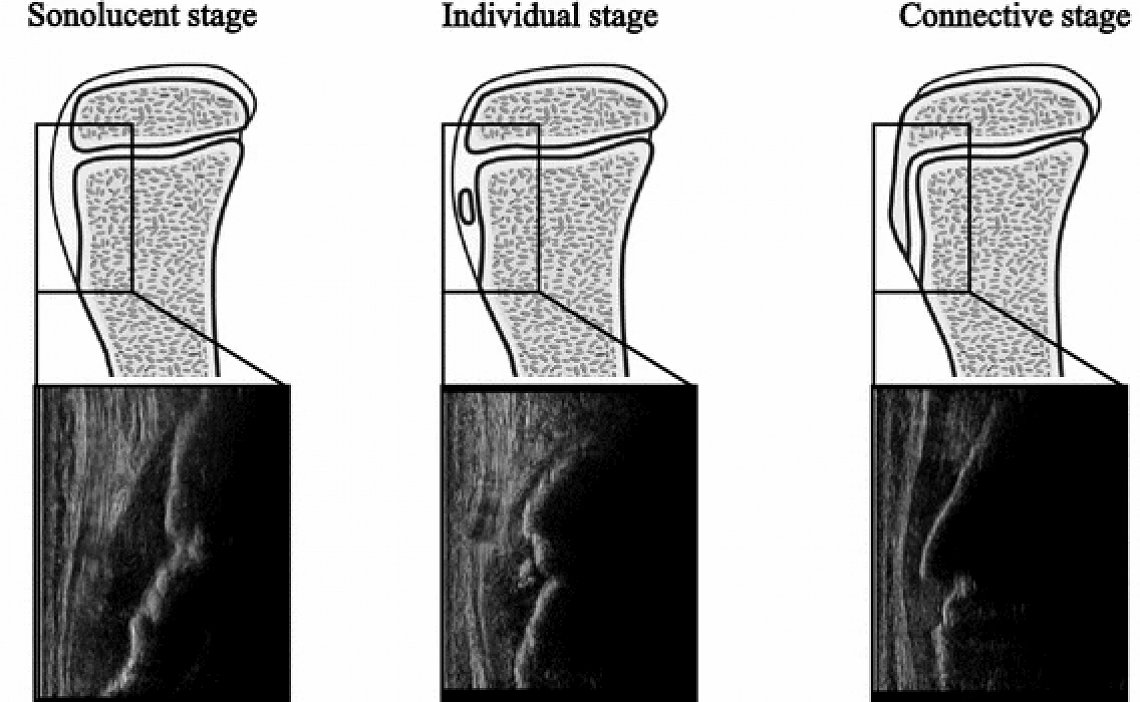
It has been suggested that OSD is caused by overuse in the period of stage I, where the tibial tuberosity changes dramatically in the short period between these stages (Nakase et al., 2015).
Factors to consider in OSD
Factors include:
1. Increased quadricep femoris muscle tightness
2. Increased knee extension strength
3. Concomitant tightness of hamstrings and triceps surae muscle
4. Reduced core stability and lower extremity flexibility (occurs especially during rapid growth spurts)
5. Sudden increase in physical activity load
6. Growth spurt
How can we manage OSD?
OSD is a self-limiting condition that settles at the time of bony fusion of the tibial tubercle. 90% of patients have complete resolution of symptoms with conservative management, making it the first-line of treatment for OSD.
How do we appropriately load patients with OSD?
Activity modification is key to managing adolescents with OSD. More often than not, adolescents are involved in multiple sports. Given that, they can consider reducing or eliminating one or two sports that they might be involved in. Activity limitation should be guided by pain. On top of that, it has been shown that a reduction in activity will improve pain levels. There is no evidence that rest accelerates the healing process, hence it is encouraged that adolescents with OSD continue to engage in their sport, with appropriate load modifications.
Physiotherapy management of OSD
Symptomatic management is the main approach to managing adolescents with OSD. It is pivotal we do a thorough assessment to identify any impairments that might be present in the patient.
Common impairments include:
1. Tight and weak hamstrings muscles
2. Tight and weak quadricep muscles
3. Biomechanical abnormalities such as excessive subtalar pronation
Hence, a wide variety of exercises should be used to address the different impairments.
Examples of exercises that may be prescribed include:

Hamstring stretch for tight hamstrings

Quadriceps stretch for tight quadriceps

Hip hitch to target weak gluteus medius muscle

Towel toe crunches to address excessive subtalar pronation
Other differential diagnoses that we should not miss!
There are many other possible causes for anterior knee pain and a thorough assessment, coupled with appropriate scans should be conducted to rule out other possible conditions such as:
Sinding-Larsen-Johansson Syndrome (SLJ)
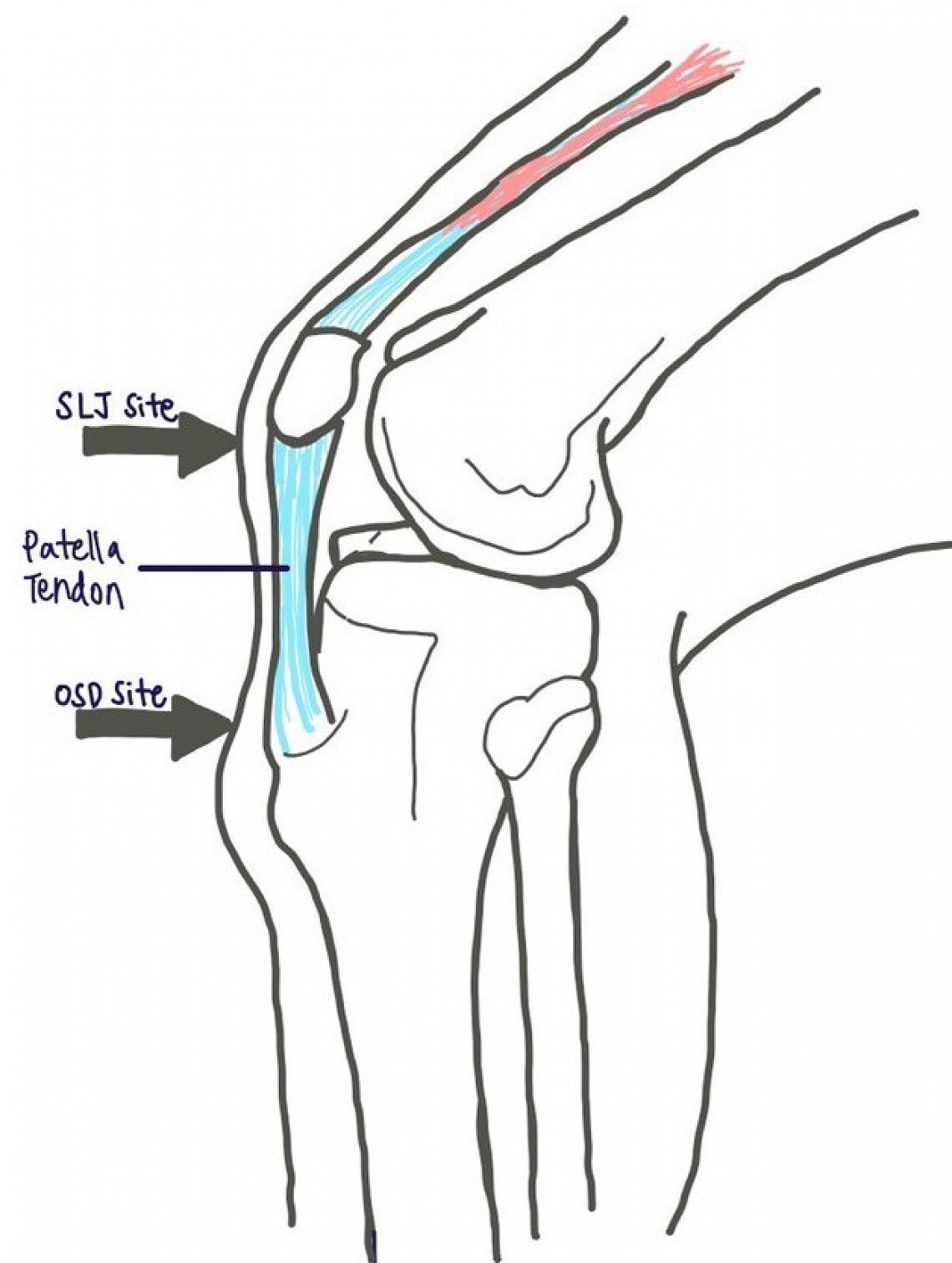
Sinding-Larsen-Johansson (SLJ) Disease is a condition similar to OSD and presents with pain in the anterior knee. However in SLJ, it is the proximal attachment of the patella tendon that is affected and causes traction apophysitis of the inferior patella pole. Diagnosis is made clinically with tenderness over the inferior pole of the patella and x-rays may show a spur at the inferior pole of the patella. Like OSD, it is more common in adolescents and due to overuse.
Patellofemoral joint pain (PFJP)
6-7% of adolescents, aged 15-19 years suffer from patellofemoral joint pain (PFJP). It may manifest due to high training loads. Many adolescents do not reduce their training load despite pain, due to the integral nature of sport to their life. This can lead to PFJP. Adolescents with PFJP may complain of increased pain with increased knee flexion (eg. going up higher steps).
Patella tendinopathy
Patellar tendinopathy is an overuse injury and is a cause of anterior knee pain. Tenderness may be present on palpation at the distal pole of patella in full extension. It is common in adolescents who are involved in jumping sports and presents with insidious onset of localised pain on the inferior pole of the patella.
Osteochondritis Dissecans
Osteochondritis dissecans generally present with intermittent pain and gradual onset of swelling. Occasionally, there may be acute painful locking of the knee. Its acute presentation is associated with hemarthrosis and loose body formation and an MRI may be useful to reveal any evidence of loose bodies or defect at the lateral aspect of the medial femoral condyle.
Referred pain from the hip
In any young athlete presenting with knee pain, it is necessary to clear the hip of any pathology such as a slipped capital femoral epiphysis or Perthes disease. These conditions commonly present as knee pain due to the innervation by the obturator nerve.
References:
Nakase, J., Goshima, K., Numata, H., Oshima, T., Takata, Y., & Tsuchiya, H. (2015). Precise risk factors for Osgood–Schlatter disease. Archives of orthopaedic and trauma surgery, 135(9), 1277-1281.