The ultimate goal of Physiotherapy is to help patients return to their desired activity goals, whether it is competitive sports or functional activities. Helping them gain the confidence to do those activities is just as important as ensuring that they are physically ready for the demands of the activity.
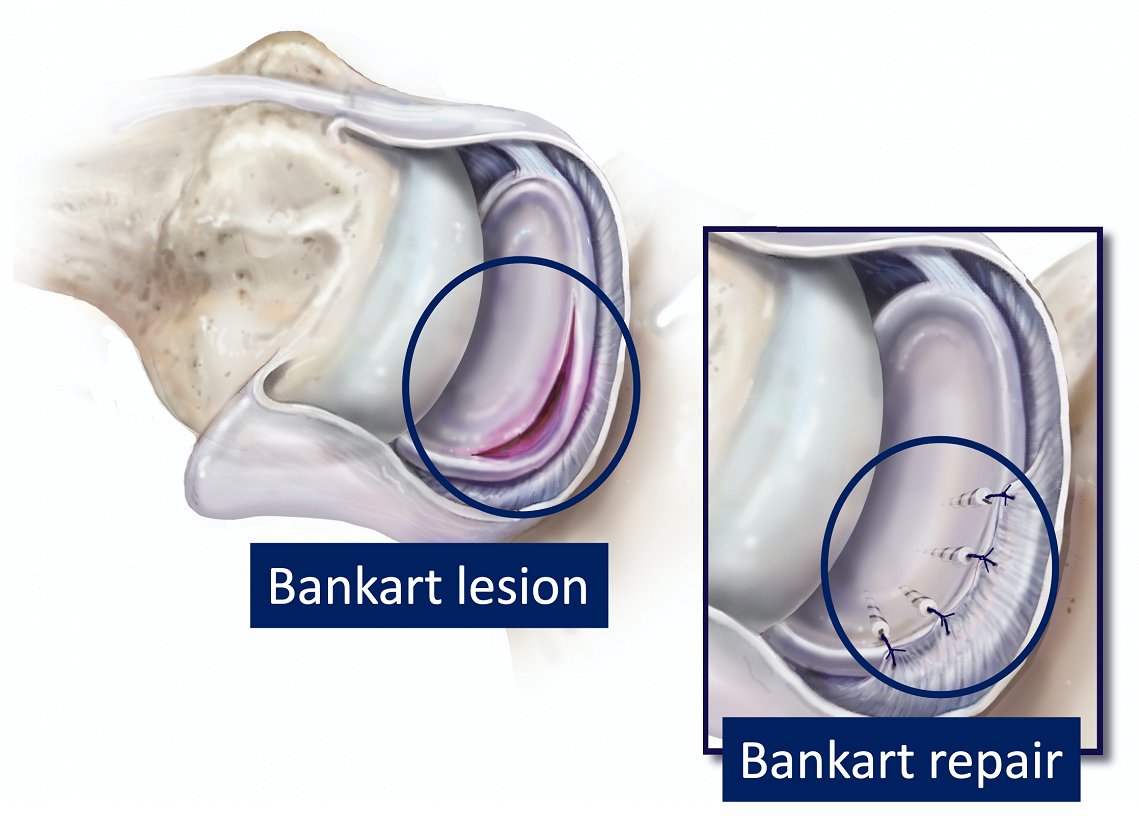
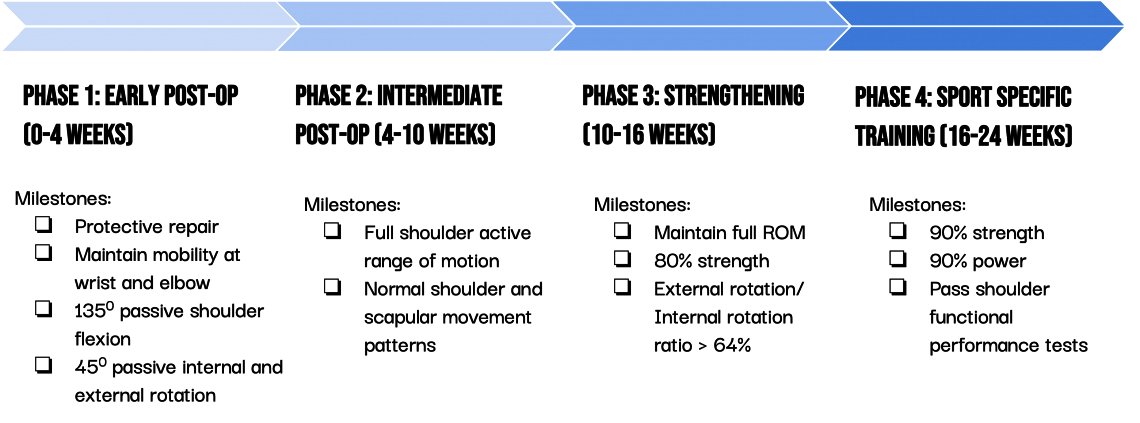
Post Bankart repair rehabilitation can be broadly categorised into 4 phases:
| Phase | Goals | Suggested exercises | Rationale |
|---|---|---|---|
| Early post-op (0-4 weeks) | – Protect the repair
– Maintain mobility of the shoulder, elbow and wrist |
1. Shoulder AROMs (e.g. supported pendulum swings, assisted shoulder flexion, etc.)
2. Active elbow and wrist movements 3. Low load scapular mobility exercises (e.g. shoulder shrugs, scapula retraction, etc.) |
While active movements are restricted in the early phase, shoulder PROMs are necessary to minimise stiffness while protecting the repair. This will help in restoring ROM later in rehabilitation, leading to better outcomes. |
| Intermediate post-op (4-10 weeks)/td> | – Regain full shoulder range of motion
– Restore muscle strength – Normalise arthrokinematics and improve neuromuscular control |
1. Shoulder AROMs and stretching
2. Low load strengthening exercises for muscles around the shoulder 3. Low load stability exercises (eg. Swiss ball high plank against the wall) 4. Upper limb PNF exercises |
After 4 weeks, the patient is allowed to engage in active shoulder movements. Hence, more aggressive exercises should be used to regain full shoulder range of motion.
Starting with gentle upper body strengthening exercises is essential to restore strength in the affected limb. A comprehensive rehabilitation program should include exercises that target the following key muscle groups: 1. Dynamic stabilisers of the shoulder (e.g. rotator cuff muscles) However, the use of heavy weights, performing exercises at end range or to fatigue is contraindicated at this stage. |
| Strengthening phase (10-16 weeks | – Ensure full shoulder ROM
– Shoulder strength 70-80% of unaffected side – Improve functional performance of upper extremity |
1. Progress shoulder strengthening exercises
2. High load chain stability exercises (e.g. Bosu ball high plank on the ground) |
By now, patients should have achieved full ROM. Hence, we can progress on to more aggressive strengthening exercises involving heavier weights and movements through full range of motion.
Another important aspect that must not be neglected in rehabilitation is to train static and dynamic stability of the shoulder. |
| Sport-specific training (16-24 weeks) | – Muscle strength > 90% of non-injured arm
– Muscle power > 90% of non-injured arm – Improve upper limb functional performance in sporting movements |
1. Continue progressing shoulder strengthening exercises
2. Shoulder power exercises (e.g. med ball throws, plyometric exercises) 3. Reactive stability exercises (e.g. reactive ball catches in abduction) |
Since the demands on the body are unique in different sports, the exercises in this phase can vary significantly between athletes.
However, the common goal is to prepare the athlete for the demands of their sport in a safe and controlled environment. This is done through building sufficient strength, power, stability and neuromuscular control. |
Early post-op exercises:

Assisted shoulder flexion
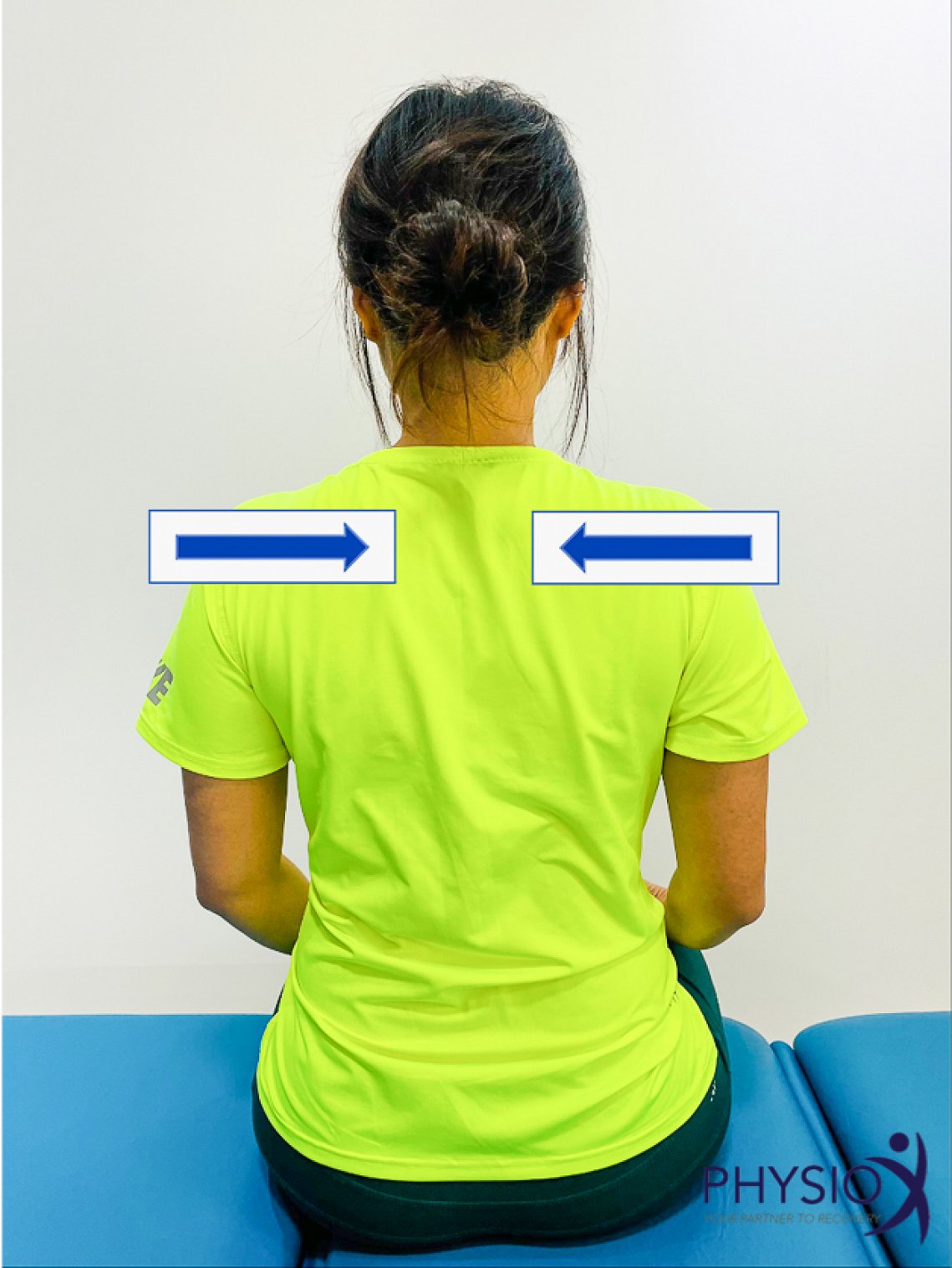
Shoulder retractions
Intermediate post-op exercises:

Wall slides with over pressure

Isometric internal and external rotations

Scapula push ups

Light resistance shoulder flexion
Strengthening phase exercises:

Dumbbell lateral raise

Resisted shoulder internal rotation

Resisted shoulder external rotation

Prone ‘I’, ‘Y’ and ‘T’s

Bosu ball shoulder stability
Sport-specific training exercises:

Overhead med ball throws

Plyometric ball catches in external rotation
When is the athlete ready to return to sport?
While 6 months post-op has traditionally been deemed as an appropriate time for return to sport, a criteria-based decision making process is understandably gaining more popularity. The following criteria can be considered:
- Pain free full range of motion
- Muscle strength and endurance > 90% of non-injured arm
- E.g. External Rotation Endurance Test (ERET)
- Pass functional assessment
- E.g. Closed Kinetic Chain Upper Extremity Stability Test (CKCUEST)
- E.g. Unilateral seated shot put test
Examples of return to sport assessment:

Unilateral seated shot put test

Closed Kinetic Chain Upper Extremity Stability Test (CKCUEST)